

TL;DR
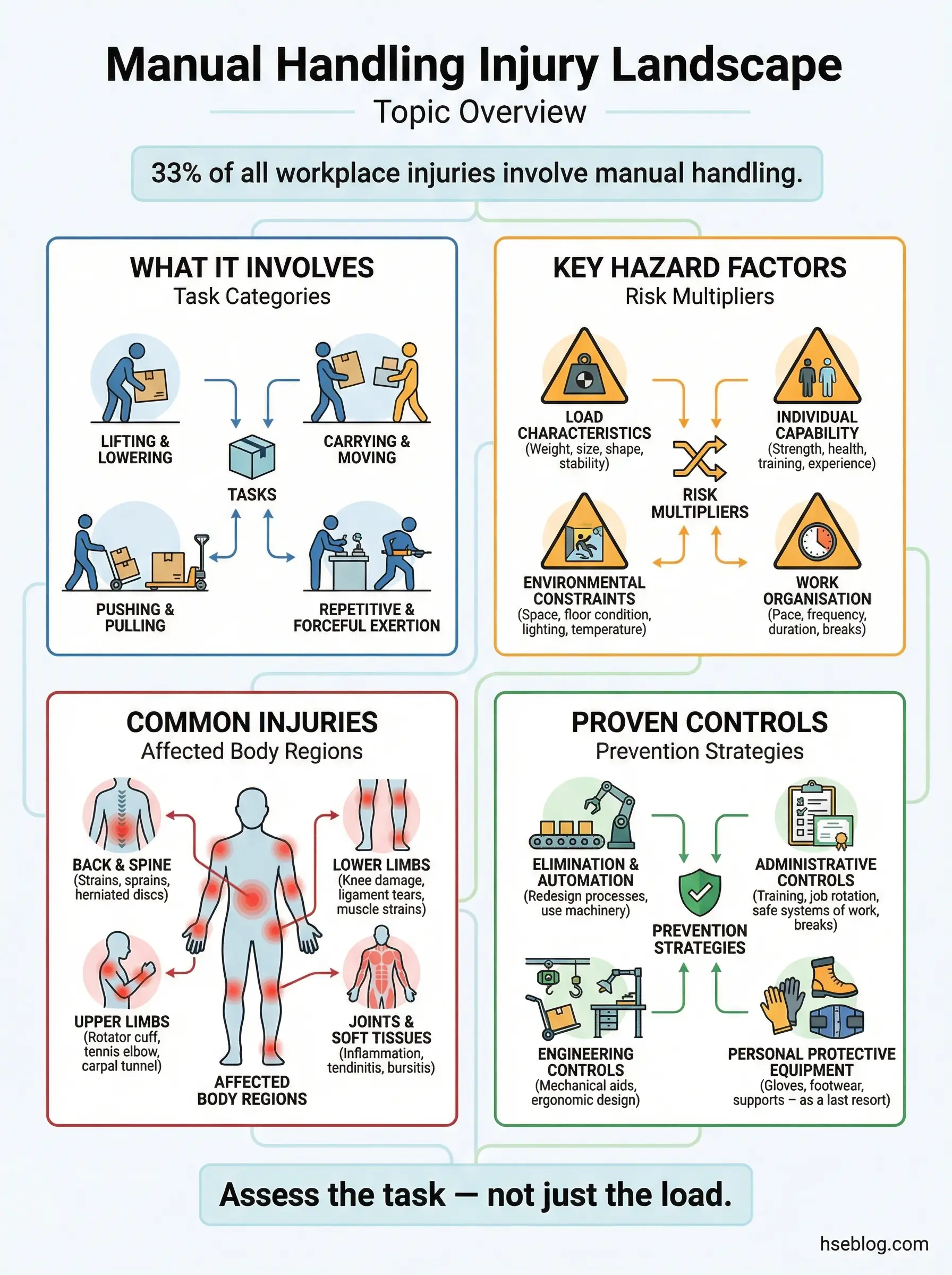
- Manual handling causes over one-third of all workplace injuries — and nearly every one is preventable with proper technique and task design
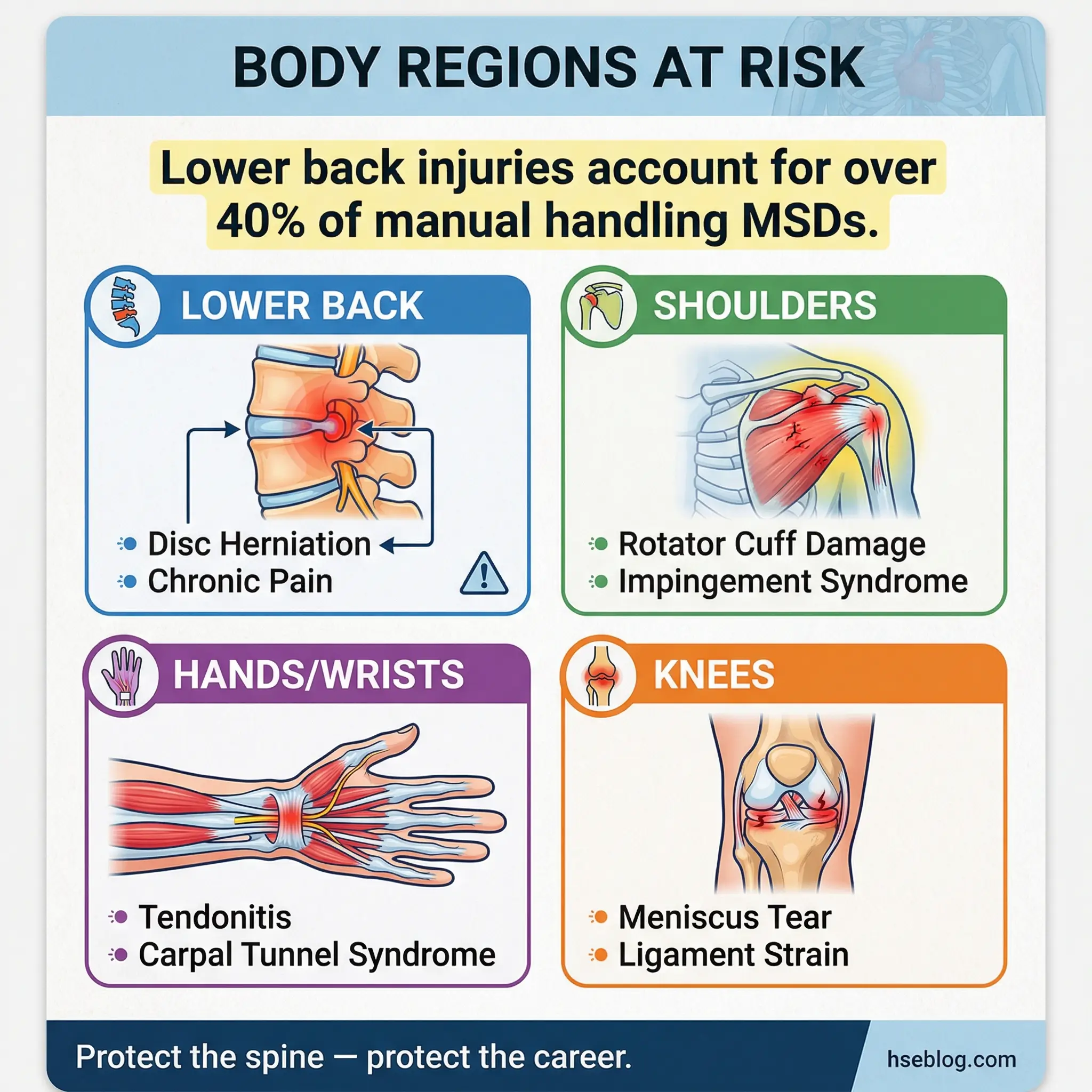
- Back injuries are the most common result but hands, shoulders, knees, and necks are equally at risk during repetitive or awkward lifts
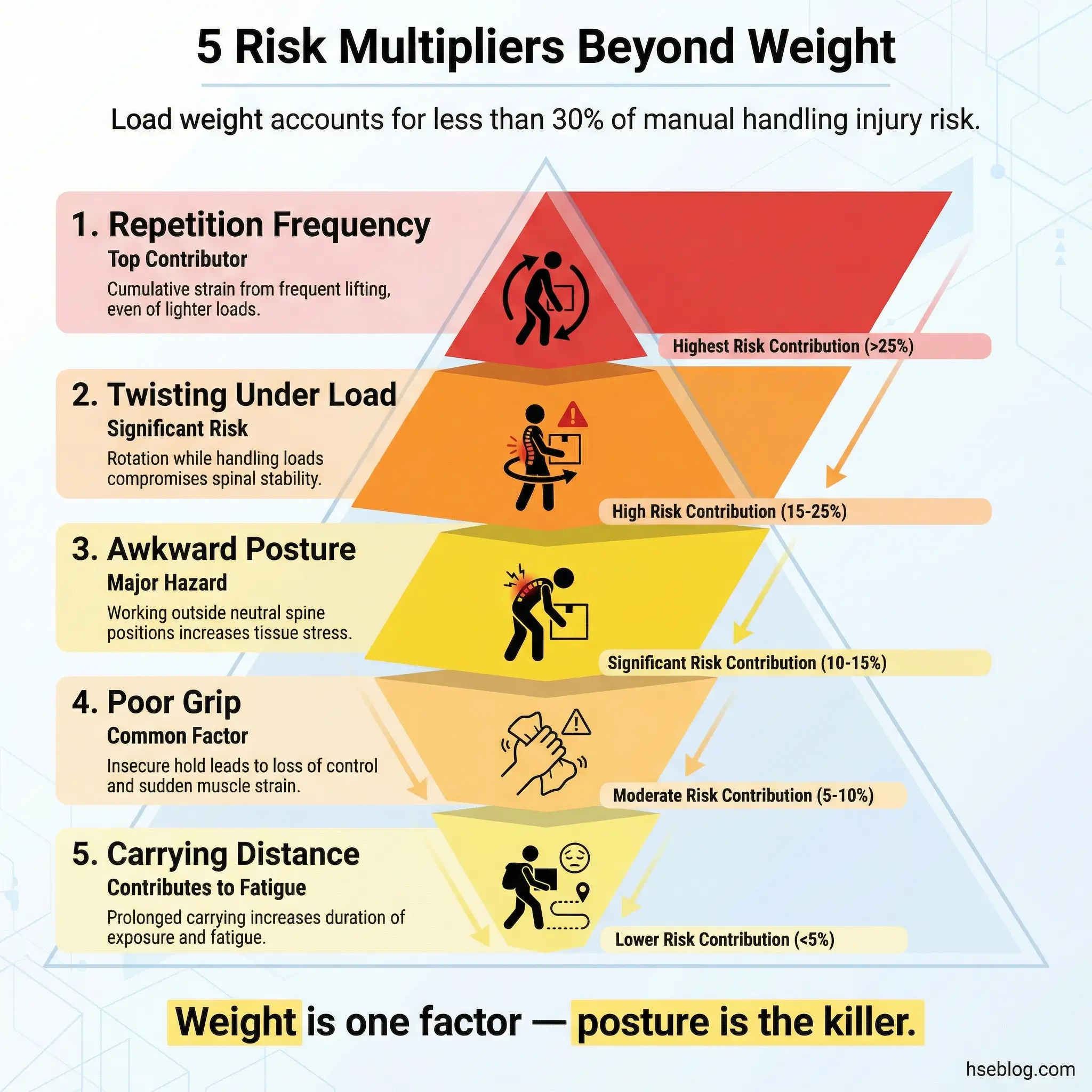
- The hazard isn’t just heavy loads — frequency, posture, grip, distance, and environment multiply risk faster than weight alone
- Risk assessment before the task starts is the single most effective control — not training after someone is already hurt
- Mechanical aids, job redesign, and team lifting eliminate more injuries than any amount of “lift with your legs” coaching ever will
I was walking through a warehouse in Southeast Asia when I saw a worker drop to one knee mid-lift. He wasn’t carrying anything unusually heavy — a 15-kilogram box of fasteners. But he’d been doing it for three straight hours without rotation, bending and twisting from a pallet on the ground to a shelf at chest height. His lower back seized. He couldn’t straighten up. Two coworkers helped him to the site clinic, and he didn’t return to work for six weeks.
That incident stays with me because it captures what most people get wrong about manual handling. They think the danger is a single heavy lift. It rarely is. The real damage comes from repetition, poor posture, bad task design, and a culture that treats manual handling as too simple to assess. Musculoskeletal disorders from manual handling remain the leading cause of workplace absence globally, costing industries billions annually in lost productivity, medical treatment, and compensation claims. This article breaks down what manual handling actually involves, the specific hazards and injuries it creates, the mistakes that keep causing them, and the practical controls that work on real job sites.
What Is Manual Handling and Why Does It Matter?
Manual handling is any activity that requires a person to use physical force to lift, lower, push, pull, carry, hold, or restrain a load. The load can be an object, a person, or an animal. It includes obvious tasks like stacking pallets and less obvious ones like holding a drill overhead for twenty minutes or pushing a loaded trolley across uneven ground.
The definition matters because most workplaces dramatically undercount their manual handling tasks. They focus on warehouse picks and construction lifts while ignoring the nurse repositioning a patient, the office worker moving boxes of printer paper, or the maintenance technician pulling cable through a ceiling void. Every one of these tasks carries musculoskeletal risk.
Under the UK Manual Handling Operations Regulations 1992 (as amended), employers must avoid hazardous manual handling operations where reasonably practicable, assess any that cannot be avoided, and reduce the risk of injury as far as reasonably practicable.
OSHA addresses manual handling primarily through the General Duty Clause (Section 5(a)(1)) and ergonomic guidelines for specific industries, since no single comprehensive manual handling standard exists in the US framework. The European Union’s Council Directive 90/269/EEC sets minimum health and safety requirements for manual handling across all member states. Regardless of jurisdiction, the legal obligation is consistent: assess, control, and monitor.
Pro Tip: When auditing manual handling on site, don’t just ask “what do you lift?” Ask workers to walk you through their entire shift sequence. The tasks they forget to mention — the repetitive ones, the awkward reaches, the sustained holds — are usually the ones causing damage.
Common Manual Handling Hazards That Lead to Injury
The weight of a load gets all the attention. But in my experience investigating manual handling injuries across construction, logistics, and petrochemical operations, weight alone rarely tells the full story. Five interconnected hazard factors determine whether a task is safe or damaging.
The Load Itself
Not every hazardous load is heavy. The characteristics of what’s being handled create risk independent of weight.
- Unstable or shifting contents — liquids in drums, loose materials in bags, and unevenly packed boxes shift the center of gravity mid-lift, forcing sudden muscular corrections that strain the lower back
- No grip points — smooth, wide, or wet surfaces force workers to grip harder and hold loads away from the body, dramatically increasing spinal compression forces
- Bulky dimensions — loads wider than shoulder width or taller than eye level force awkward postures and block forward vision, increasing the risk of trips and collisions
- Sharp edges or hot surfaces — workers instinctively hold hazardous loads away from the body, multiplying the lever arm on the spine
The Task Design
How a manual handling task is structured often matters more than what’s being moved. I’ve seen operations where the load was well within guideline weights but the task design guaranteed injury over time.
- High-frequency repetition — performing the same lift-lower cycle more than 12 times per hour without rotation increases cumulative tissue fatigue beyond recovery capacity
- Twisting under load — any task that requires turning the torso while holding weight generates shear forces across lumbar discs, the single most common mechanism for disc herniation
- Extended carrying distances — carrying loads beyond 10 meters significantly increases grip fatigue and changes gait patterns, raising both musculoskeletal and slip-trip-fall risk
- Working above shoulder height or below knee level — these postural extremes reduce available muscle strength by 30–50%, forcing the spine to compensate
The Working Environment
Even a well-designed task with a manageable load becomes dangerous when environmental conditions are poor. These are the factors I flag most often during site walk-throughs.
- Uneven or slippery floors — workers adjust their posture to maintain balance, often unconsciously, which compromises lifting mechanics and increases fall-while-carrying incidents
- Confined or cluttered spaces — restricted room forces workers into bent, twisted, or crouched postures and limits their ability to use proper technique
- Poor lighting — dim work areas cause misjudged loads, missed steps, and delayed hazard recognition
- Extreme temperatures — cold environments reduce muscle flexibility and grip sensitivity; hot environments accelerate fatigue and reduce concentration
- Changes in floor level — ramps, steps, and dock edges during carrying tasks multiply the risk of trips and overexertion
Individual Capability
The same task that one worker performs safely can injure another. Individual factors don’t excuse poor task design, but ignoring them leads to preventable harm.
- Pre-existing musculoskeletal conditions — previous back injuries, shoulder problems, or joint conditions reduce tolerance for manual handling loads
- Fitness and conditioning — workers returning from extended leave, new starters, and aging workforce members require adjusted task allocation
- Insufficient training — workers who have never been taught body mechanics default to the most intuitive (and most dangerous) lifting patterns
- Fatigue from shift patterns — manual handling injury rates spike in the last two hours of long shifts and during night work
Pro Tip: During risk assessments, I always check the task at the end of a shift, not the beginning. Workers compensate well when they’re fresh. The real hazard profile shows up at hour ten.
Manual Handling Injuries: What Gets Damaged and How
Manual handling injuries are not a single category. They range from acute traumatic events to slow-onset conditions that develop over months or years. Understanding the injury types helps target prevention where it matters most.
Musculoskeletal Disorders (MSDs)
MSDs are the signature injury of manual handling. They affect muscles, tendons, ligaments, joints, nerves, and spinal discs. These are the conditions that drive the majority of workers’ compensation claims and long-term disability in manual-handling-intensive industries.
- Lower back injuries — disc herniation, lumbar sprains, and chronic low back pain account for the largest share of manual handling MSDs; the L4-L5 and L5-S1 disc levels are most frequently damaged by combined flexion and rotation under load
- Shoulder injuries — rotator cuff strains and tears from overhead lifting, repetitive reaching, and sustained holds above shoulder height
- Knee injuries — meniscus damage and ligament strain from lifting while crouching, kneeling on hard surfaces, or rising from deep squats under load
- Neck and upper back injuries — cervical and thoracic strain from sustained awkward head positions during carrying tasks or overhead work
- Hand and wrist injuries — carpal tunnel syndrome, tendonitis, and De Quervain’s tenosynovitis from repetitive gripping, pinching, and force application
Acute Traumatic Injuries
Not all manual handling injuries develop gradually. Sudden failures happen, and they’re often severe.
- Herniated discs — a single heavy or awkward lift can rupture a spinal disc instantly, causing immediate radiating pain, numbness, and in severe cases, loss of bladder or bowel function
- Muscle tears — sudden overexertion or jerking movements tear muscle fibers, most commonly in the lower back, biceps, and hamstrings
- Crush injuries — dropped loads landing on feet, hands, or lower limbs can fracture bones and damage soft tissue
- Fractures — falls while carrying loads frequently result in wrist, hip, and ankle fractures, particularly in older workers
Cumulative vs. Single-Event Injuries
This distinction matters enormously for prevention strategy. I’ve watched too many organizations focus all their controls on preventing the dramatic single-event injury — the heavy lift that breaks a back — while ignoring the slow accumulation of tissue damage from thousands of moderate lifts performed with poor technique.
Cumulative injuries are harder to attribute, harder to report, and harder to claim. Workers often don’t recognize them until the damage is advanced. By the time a warehouse operative reports chronic low back pain after two years of daily pallet work, the L5-S1 disc has been degrading for months. Prevention for cumulative injuries requires job rotation, task redesign, and proactive health surveillance — not just safe lifting posters on the break room wall.
Common Mistakes That Cause Manual Handling Injuries on Site
After years of auditing manual handling operations, I’ve compiled a pattern of failures that repeat across industries. These aren’t theoretical risks. Each one comes from an actual incident or near-miss I’ve documented.
The following mistakes appear in incident reports far more often than any worker wants to admit — and they’re almost entirely preventable with better planning and supervision.
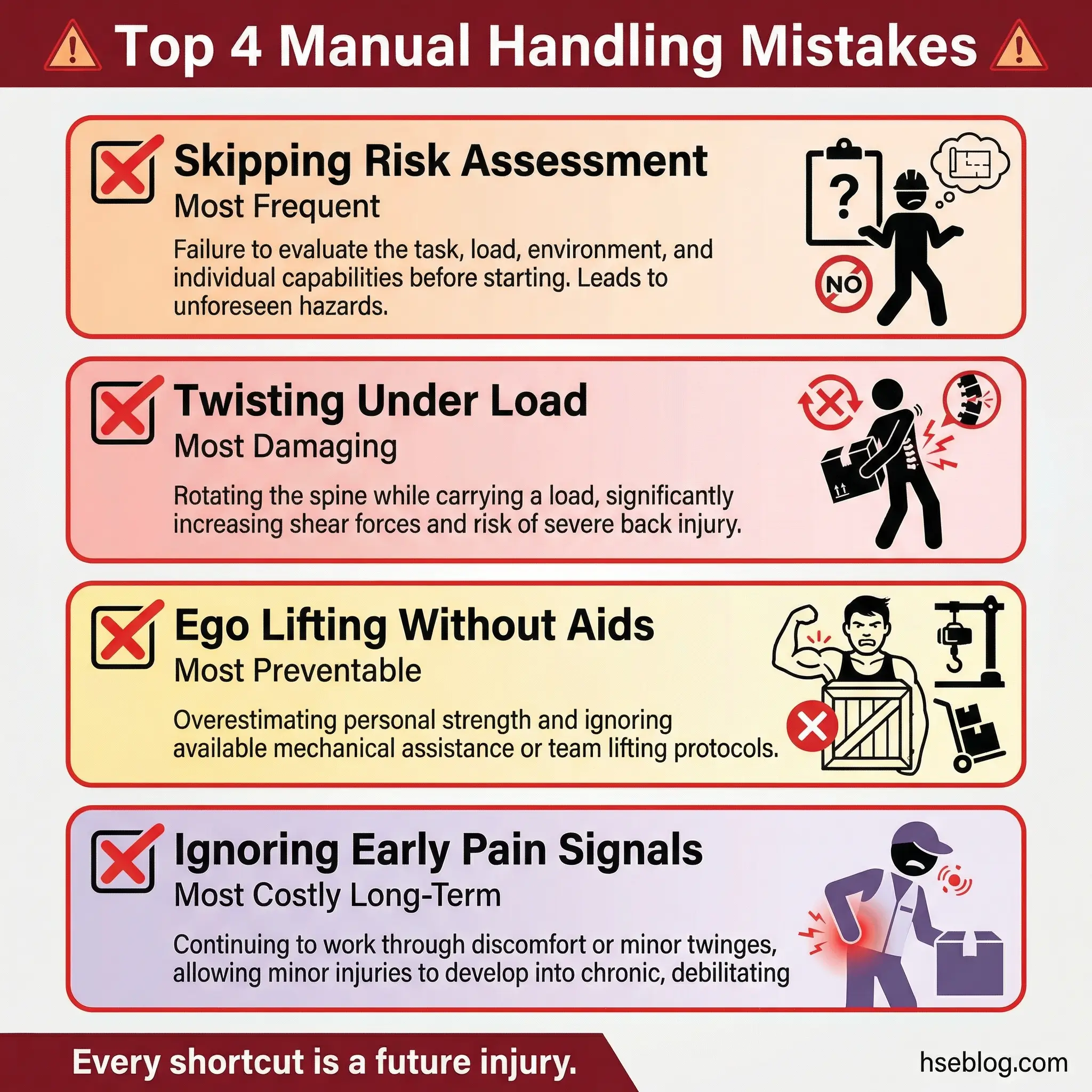
- Skipping the risk assessment — the most common failure; workers begin lifting without any consideration of load weight, path of travel, destination height, or their own physical condition
- Ego lifting — refusing help or mechanical aids to appear capable; this kills more backs than any hazard on site
- Twisting instead of turning feet — rotating the torso while holding a load generates the highest shear forces on lumbar discs; proper technique requires pivoting with the feet, not the spine
- Lifting from the floor to overhead in one motion — this demands the spine move through its maximum range under load; every intermediate rest point eliminated is a risk multiplied
- Gripping too tightly on smooth loads — excessive grip force fatigues forearm muscles and tendons rapidly, leading to dropped loads and chronic tendon injury
- Ignoring early warning signs — mild stiffness, tingling, or aching after shifts are the body’s early damage signals; workers who push through these routinely progress to serious MSDs within months
- Carrying loads that block forward vision — this eliminates hazard awareness and has caused fatal falls from dock edges and into open excavations
Pro Tip: Install full-length mirrors at manual handling stations so workers can see their own posture during lifts. Self-correction is faster and more effective than any verbal coaching.
| Common Mistake | What Actually Happens | Likely Injury |
|---|---|---|
| No risk assessment | Worker misjudges load or path | Acute back strain, crush injury |
| Twisting under load | Shear forces on lumbar discs | Disc herniation |
| Lifting floor to overhead | Maximum spinal range under load | Shoulder tear, spinal compression |
| Carrying with blocked vision | Trip or fall while loaded | Fracture, head injury |
| Ignoring early symptoms | Cumulative tissue degradation | Chronic MSD, disability |
Practical Control Measures for Manual Handling Hazards
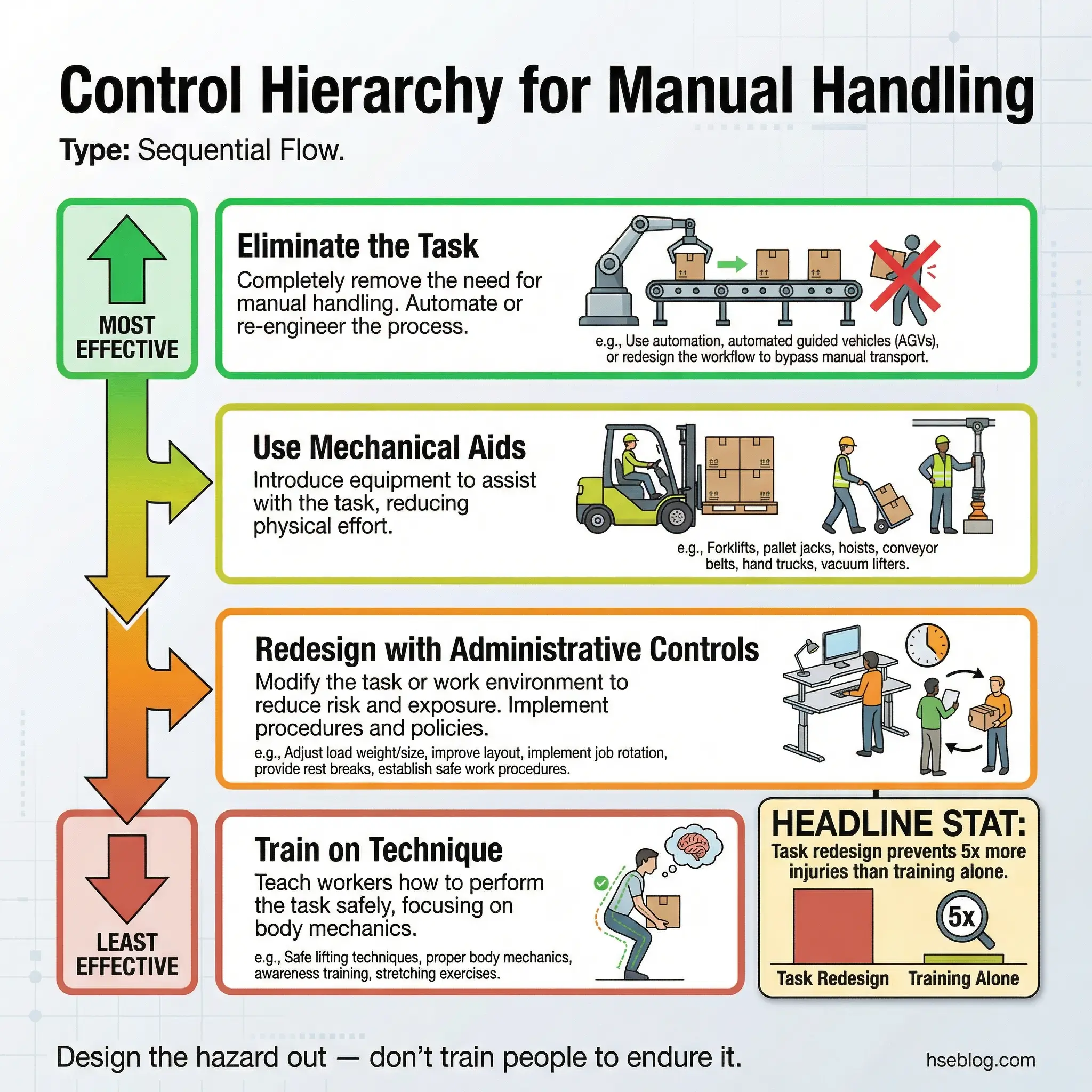
Controls that actually reduce manual handling injuries follow a clear hierarchy. The most effective controls eliminate the handling task entirely. The least effective — and most commonly relied on — are training and PPE. Every organization I’ve audited over-invests in training and under-invests in task redesign.
Elimination and Redesign
The only guaranteed way to prevent a manual handling injury is to remove the manual handling altogether. Where that’s not possible, redesigning the task to reduce demand is the next priority.
- Automate where feasible — conveyor systems, vacuum lifters, and automated guided vehicles remove human lifting entirely from repetitive, high-volume operations
- Redesign storage layouts — position frequently handled items between knee height and shoulder height (the “power zone”) to eliminate bending and overhead reaching
- Reduce load weights — repackage materials into smaller units; a 25 kg bag of cement split into two 12.5 kg bags halves the spinal load per lift
- Shorten carrying distances — relocate storage closer to work areas; every meter eliminated reduces cumulative fatigue and exposure time
- Use gravity-fed systems — roller conveyors, chutes, and tilt tables let gravity do the work that a human spine shouldn’t
Mechanical Aids and Equipment
When elimination isn’t practical, mechanical aids bridge the gap between what the task demands and what the human body can safely deliver.
- Pallet jacks and powered trolleys — essential for horizontal movement of loads over 20 kg or across distances greater than 10 meters
- Scissor lift tables — bring the load to optimal working height, eliminating bending and floor-level lifts
- Vacuum lifters and suction cups — handle smooth, flat loads (glass, sheet metal, panels) without requiring grip force
- Hoists and davit cranes — manage vertical lifts in confined or restricted access areas where forklifts cannot operate
- Patient handling slings and hoists — in healthcare settings, these are not optional; manual patient handling is the leading cause of nursing back injuries worldwide
OSHA’s Ergonomic Guidelines for Nursing Homes specifically recommend mechanical lifting devices for all patient handling tasks, noting that manual lifting of patients is inherently unsafe regardless of technique.
Administrative Controls
Administrative controls don’t change the physical task, but they change how workers interact with it. They’re essential as a supplementary layer but never sufficient alone.
- Job rotation schedules — rotate workers across manual handling and non-handling tasks every 2 hours to prevent cumulative fatigue in any single muscle group
- Mandatory rest breaks — enforce 10-minute breaks after every 60 minutes of continuous manual handling, separate from standard shift breaks
- Team lifting protocols — establish clear rules: any load above 25 kg requires two-person handling or mechanical assistance; this threshold should be enforced, not suggested
- Pre-task risk assessments — before any manual handling activity, workers should assess the load, route, destination, available aids, and their own physical readiness using a simple five-point check
- Health surveillance programs — regular musculoskeletal screening identifies early-stage damage before it progresses to chronic conditions
Training and Technique
Training sits at the bottom of the control hierarchy for a reason. I’ve never seen a manual handling injury problem solved by training alone. But combined with better task design and mechanical aids, proper technique training reduces residual risk.
The following principles should be covered in practical, hands-on training sessions — not classroom lectures with slide decks.
- Plan the lift before starting — assess the load, the path, and the destination
- Position feet shoulder-width apart, one foot slightly ahead, to create a stable base
- Bend at the hips and knees, not the waist — maintain the natural curve of the lower back
- Get a firm grip with both hands before lifting — test the load weight with a gentle push before committing
- Keep the load close to the body — the further the load from the spine, the greater the compressive force
- Lift with the legs, not the back — drive upward through the thighs and glutes
- Avoid twisting — turn by pivoting the feet, never by rotating the torso under load
- Set down by reversing the sequence — bend at the knees and hips, place the load, then release the grip
Pro Tip: The best manual handling training I’ve delivered used weighted boxes at an actual workstation — not a classroom. Workers practice with the real loads, the real heights, and the real constraints they’ll face on shift. Classroom training alone changes knowledge. Practical training changes behavior.
How to Conduct a Manual Handling Risk Assessment
A manual handling risk assessment is the foundation for every control measure. Without it, controls are guesses. With it, resources go exactly where the risk is highest. The process I use on site follows a structured but practical sequence that any competent supervisor can apply.
Every manual handling risk assessment should evaluate four interconnected factors — the task, the load, the environment, and the individual. Regulators often refer to this as the TILE framework.
- Identify all manual handling tasks — walk the operation end to end and list every activity involving human force application; include pushing, pulling, carrying, holding, and restraining, not just lifting
- Assess each task against the TILE factors — for each task, document the Task demands (frequency, duration, posture, distance), the Load characteristics (weight, stability, grip), the Individual capability (training, fitness, history), and the Environment conditions (space, flooring, temperature, lighting)
- Score the risk level — use a risk matrix to rate each task based on likelihood and severity of potential injury; prioritize tasks scoring high on both dimensions
- Identify and implement controls — apply the hierarchy: eliminate first, then redesign, add mechanical aids, administrative controls, and finally training
- Record and communicate findings — document the assessment, brief all affected workers, and post control requirements at the workstation
- Review and update — reassess whenever the task changes, after any manual handling injury, and at minimum annually
| TILE Factor | What to Assess | Red Flags |
|---|---|---|
| Task | Frequency, posture, distance, duration | >12 lifts/hour, twisting, floor-to-overhead, >10m carry |
| Individual | Training, fitness, health, experience | New starter, returning from injury, night shift fatigue |
| Load | Weight, stability, grip, dimensions | >25 kg, no handles, shifting contents, bulky |
| Environment | Space, flooring, lighting, temperature | Wet floors, confined area, poor lighting, extreme heat/cold |
The Real Cost of Ignoring Manual Handling Hazards
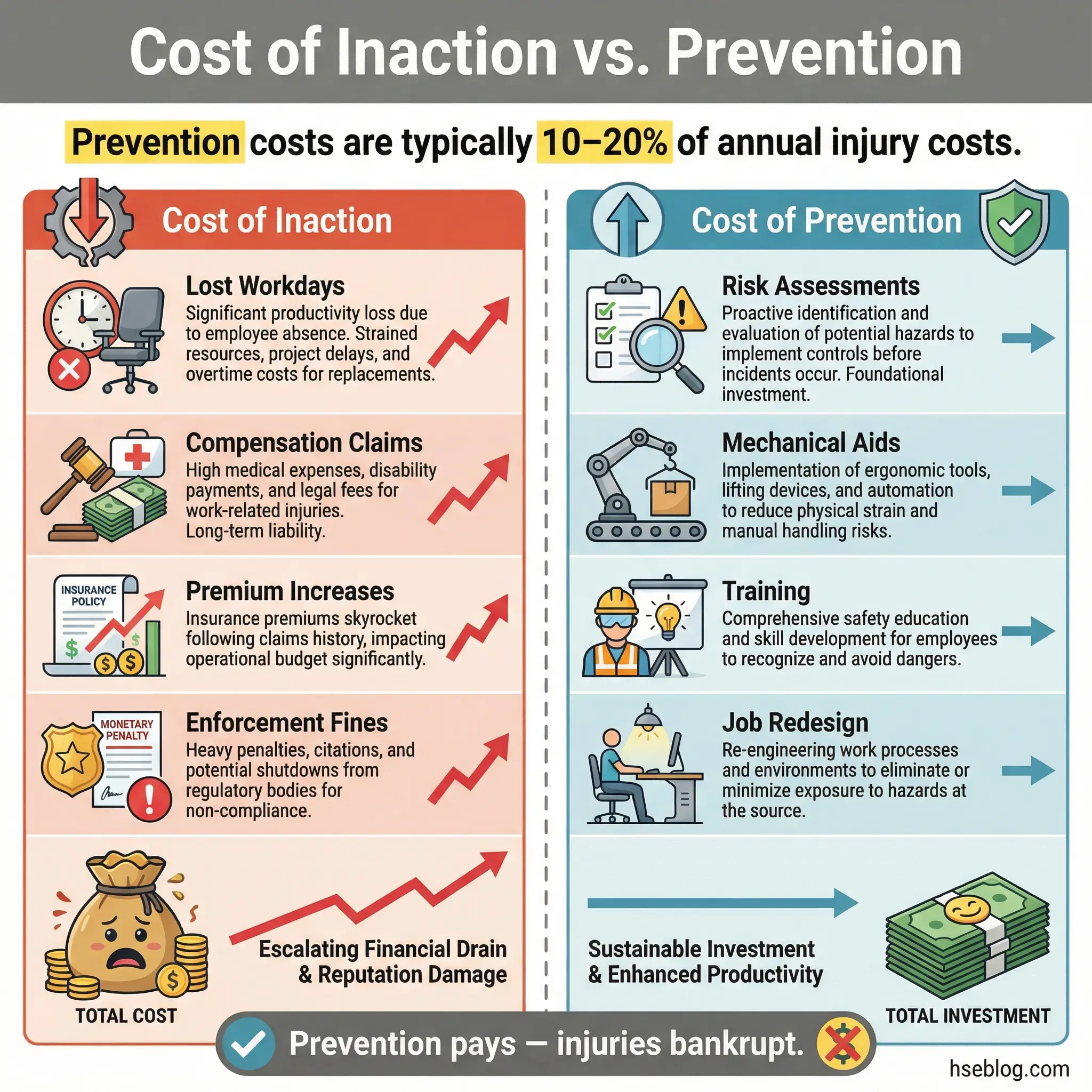
Organizations that treat manual handling as a low-priority, “common sense” issue pay for it — repeatedly. The direct and indirect costs of workplace accidents from manual handling injuries compound rapidly and extend far beyond the injured worker.
- Workers’ compensation claims — back injuries alone generate some of the highest average claim costs in most compensation systems, often exceeding $40,000 per case for surgical interventions
- Lost productivity — each manual handling injury resulting in lost time costs the employer an average of 12 days of absence; chronic MSDs cost months or years
- Replacement and retraining costs — covering an injured worker’s absence requires overtime, temporary staffing, and productivity losses during the learning curve
- Regulatory enforcement — OSHA citations under the General Duty Clause for ergonomic hazards carry per-violation penalties; repeat or willful violations multiply the figure significantly
- Litigation exposure — employees who develop chronic conditions from years of uncontrolled manual handling have pursued — and won — substantial civil claims against employers
- Reputational damage — high MSD rates signal poor management to clients, regulators, and prospective employees
I once consulted for a logistics operation that had dismissed manual handling training and assessment as “unnecessary overhead.” In one calendar year, they recorded 23 back injuries, 4,100 lost work days, and over $800,000 in direct costs. Their insurance premiums doubled the following year. The risk assessments and mechanical aids they eventually implemented cost less than a single quarter’s injury bill.
Conclusion
Manual handling injuries are the most common, most predictable, and most preventable category of workplace harm. Every incident I’ve investigated traces back to the same root failures: no assessment was done, the task was poorly designed, mechanical aids were available but not used, or workers were never shown what proper technique looks like in their actual work environment. The fix is never a single action. It’s a system — assess every task, redesign the worst ones, provide the right equipment, train on real-world technique, and monitor for early signs of damage before they become permanent disabilities.
The reason manual handling keeps injuring people is not complexity. It’s familiarity. Organizations assume that because everyone lifts things every day, no special attention is needed. That assumption fills rehabilitation clinics and compensation files. A back doesn’t care whether the lift was at work or at home, whether the load was 10 kilograms or 30, whether it was the first lift of the day or the five-hundredth.
Every worker on your site will go home today and pick up a child, carry groceries, or bend to tie a shoe. The techniques and task designs you put in place at work determine whether they can still do those things at sixty. That’s the real measure of a manual handling program — not the audit score, not the training completion rate, but whether your people leave the job with the same body they started with.